Dr Chris Murray discusses findings and future of Global Burden of Disease study at NIH
January / February 2016 | Volume 15, Issue 1

Photo by Daniel Sone for NIH
Dr. Christopher Murray discusses insights from the
Global Burden of Disease study and new directions for the
project.
By Shana Potash
The risk factors and diseases that threaten health globally have changed significantly in the past few decades, as highlighted by the latest Global Burden of Disease (GBD) study.
The rise in noncommunicable diseases; scientific debates that come with assessing the world's health; and future plans for the GBD project were the focus of a
recent NIH talk by Dr. Christopher Murray. He is a founder of the GBD program and director of the
Institute for Health Metrics and Evaluation (IHME) at the University of Washington.
Insights on shifting disease burden
Communicable, maternal, neonatal and nutritional disorders have steadily declined around the world, while the volume of noncommunicable diseases (NCDs) has exploded, driven by population growth and an aging population. Health systems need to account for that in financing and planning, Murray said, as he presented analyses of GBD data from 1990 to 2013,
published in
The Lancet last year.
He pointed out other challenges that emerge when examining the years people spend living with disability. Back pain, diabetes, vision and hearing loss, depression and other mental health disorders are among the leading issues. But, cancer and cardiovascular disease, which are the classic causes of premature death, aren't big contributors to disability.
"What ails you, isn't necessarily what kills you," Murray explained. "It's this disconnect health systems need to deal with."
Another observation from the GBD, he noted, is the enormous role tobacco use and high blood pressure play in causing NCDs, along with unhealthy diets. In 1990, the biggest threats to health globally were malnutrition and unsafe water and sanitation. By 2013, they'd been replaced by poor diet and high blood pressure, with tobacco use not far behind.
Global Burden of Disease Study 2013:
Change in disability-adjusted life years (DALYs)
attributed to risk factors
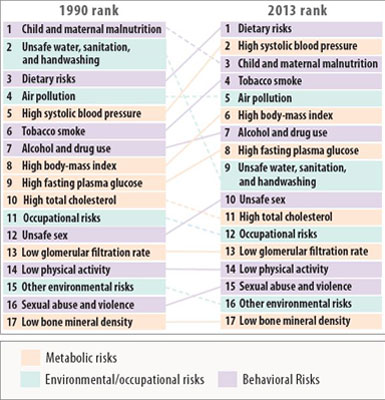
Source: IHME's
GBD Compare
Description: Arrow diagram shows the changes in disability-adjusted life
years (DALYs), attributed to risk factors, comparing the 1990 and 2013
ranks, grouping risks by metabolic, environmental/occupational and
behavioral risks. Access the full details and data using the GBD
Compare Viz Hub at
http://ihmeuw.org/3qr6.
Behavioral risk factors, followed by metabolic and environmental issues, are significant determinants of health and can explain about 40 percent of the burden globally, he observed. "I think there are important insights on the behavioral risks that are going to come from not only the epidemiology and traditional analysis of risks, but understanding how to change behavior, which of course is quite complex," he said, giving a nod to social science.
Spurring scientific and policy debates
Murray is encouraging scientists and policymakers to use
GBD data and visualization tools in their own research. The project website enables easy manipulation of data and creation of downloadable graphics. During their visit to Bethesda, Murray and his team trained 60 NIH staff on how to use the tools.
The GBD quantifies health loss from disease, injuries and risk factors by age, sex, population, and over time. It uses multiple metrics including death statistics, disease prevalence and an overall measure for the burden of disease known as disability-adjusted life years (DALYs). DALYs are the sum of years of life lost to early death and years living with disability.
There's GBD data on over 300 diseases and injuries from 188 countries back to 1990. More than 1,400 collaborators in 115 countries collect, review and analyze information from about 50,000 sources. Metadata for those sources are available in an online catalog, the
Global Health Data Exchange.
"There's a lot of complexity to trying to make sense of the world's health data," Murray commented as he described efforts to ensure content is credible, comparable and comprehensive. Uncertainty quantification, he said, is a critical component of the burden and tries to reflect uncertainty in both the model and in the underlying data.
He acknowledged recent debates around the GBD that have taken place internally among the staff, as well as externally. Hypertension was one example. The GBD asserted that risk starts when systolic blood pressure is 110-115, but some people questioned whether there really are benefits below 140-150. Murray said he was happy to see that a recent NIH study known as SPRINT found health benefits in being closer to 120, confirming the GBD analysis.
Salt was another hotly debated topic. Murray said there was no scientific agreement on the optimum daily level of sodium intake, so the GBD assessed burden was based on a range of 1-5 grams. As the science on sodium evolves, the argument for a population-level strategy to reduce intake is compelling, he noted.
Future directions for the GBD
New tools and data are in the works to provide researchers and policymakers with a more detailed picture of what's killing and ailing people, where and why.
IHME is developing mapping software to help guide the fight against the most problematic infectious diseases in low-income countries. Geospatial mapping techniques will be applied to show the disease burden of malaria, HIV, tuberculosis, diarrhea and pneumonia, as well as three neglected tropical diseases: lymphatic filariasis, onchocerciasis and human African trypanosomiasis (sleeping sickness).
The work will be similar to the
Malaria Atlas Project (MAP), Murray explained, pointing to a
recent MAP study and visualizations in
Nature that quantified the effect of malaria control efforts in sub-Saharan Africa. Dr. Simon Hay, a recent Fogarty Senior Research Fellow who co-founded MAP, is the new head of geospatial science at the IHME and is leading the effort.
A tool to forecast disease burden up to 25 years out also is being created by IHME. Users will be able to ask "what if" questions by changing the trajectory for risk or income, for example. Murray encouraged the audience to "imagine the various uses that type of forecasting tool has for giving you a background, past trends and relationships scenario to think about alternatives where your innovations here might change the course of that scenario."
GBD is moving to annual updates, with the next one planned for release in May 2016. It will include, for the first time, assessments for the U.S. by state, as well as sub-national measures for Brazil, Sweden and Japan.
Training and capacity building
Government officials in the United Kingdom, China and India are using GBD results, Murray said, and the growing interest in this type of descriptive epidemiology and data synthesis will require more training and capacity building.
"Above and beyond the traditional training in biostatistics and epidemiology, there are extra techniques and skills that need to be taught," he said, adding that the training the IHME currently provides, "is a drop in the bucket compared to what's needed."
More Information
- Watch the recorded webcast of Dr. Chris Murray's November 2015 talk,
New insights from the Global Burden of Disease 2013 study [Video], on the NIH Videocasting site, and learn more about the
November 2015 talk.
- Learn more about:
-
Access the collection of articles on the analyses of GBD data, published in
The Lancet throughout 2015:
-
Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990-2013: a systematic analysis for the Global Burden of Disease Study 2013
The Lancet, January 10, 2015 (online December 17, 2014) -
Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990-2013: a systematic analysis for the Global Burden of Disease Study 2013.
The Lancet, August 22, 2015 (online June 7, 2015) -
Global, regional, and national disability-adjusted life years (DALYs) for 306 diseases and injuries and healthy life expectancy (HALE) for 188 countries, 1990-2013: quantifying the epidemiological transition
The Lancet, November 28, 2015 (online August 26, 2015) -
Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks in 188 countries, 1990-2013: a systematic analysis for the Global Burden of Disease Study 2013
The Lancet, December 5, 2015 (online September 10, 2015)
- Learn more about the
Malaria Atlas Project, and the related publication,
The effect of malaria control on Plasmodium falciparum in Africa between 2000 and 2015, published by
Nature on October 8, 2015.
To view Adobe PDF files,
download current, free accessible plug-ins from Adobe's website.